Key Points:
- More complications with CAS than CES for carotid atherosclerosis in CKD
- Yearly increments in complication rates similar for both procedures
Among patients with chronic kidney disease (CKD), those who undergo carotid endarterectomy (CEA) have lower risk of experiencing complications than those treated with carotid artery stenting (CAS). The findings, presented October 13, 2015, at the Transcatheter Cardiovascular Therapeutics (TCT) meeting in San Francisco, CA.
Fabio V. Lima, MPH, of Stony Book Medicine (Stony Brook, NY), and colleagues used National Inpatient Sample data to identify patients with stage 5 CKD or end-stage kidney disease (ESRD) who underwent CEA (n = 1,630) or CAS (n = 511) between 2004 and 2012 for symptomatic or asymptomatic carotid artery atherosclerosis. Stage 5 CKD was defined as a glomerular filtration rate < 15mL/min/1.73 m2, and ESRD was defined as the need for dialysis.
Patients who underwent CEA were an average of 2.5 years older and more likely to be white (58.6% vs. 51.3%, P = 0.004) than those who underwent CAS. CEA patients were also more likely to have coronary artery disease (60.9% vs. 55.4%, P = 0.030) and hyperlipidemia (47.6% vs. 40.5%, P = 0.005).
The primary endpoint of in-hospital major adverse cardiovascular and cerebrovascular events (MACCE; death, acute MI, or stroke) was more common in the CAS group than in the CEA group, a difference mainly driven by higher stroke and mortality rates. There were no significant differences in the rates of GI hemorrhage or cardiac arrest/ventricular fibrillation (table 1).
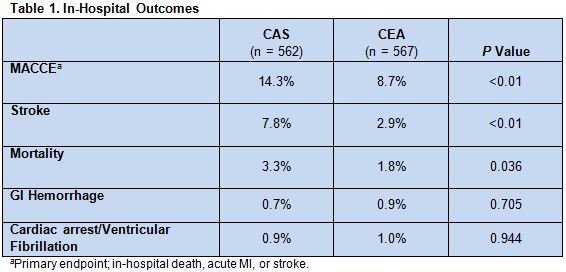
Only CAS independently predicted the occurrence of MACCE (OR 1.75, 95% CI 1.29-2.37), and yearly increment in MACCE rates was similar for both groups.
Results Dovetail With Those of CREST
“CAS has emerged as a valid alternative to CEA, [but] whether it is similar in therapeutic benefit to CEA is not without controversy,” Lima told WLNCMD in an email. “Furthermore, many previous trials comparing the 2 treatment modalities have excluded patients with moderate and severe forms of CKD and ESRD from participation in studies. Coronary revascularization studies have demonstrated evidence that these patients with higher degrees of renal impairment have more complications than those without.”
The findings mirror the CREST outcomes in that, once again, stenting is associated with a higher risk of complications, notably strokes, than endarterectomy, said Thomas Maldonado, MD, of NYU Langone Medical Center (New York, NY) in an interview with WLNCMD. “This is consistent with CREST but looking specifically at patients with renal disease, which we know is an independent poor prognosticator for all cardiovascular interventions.”
Maldonado pointed out that the study provided no information with regard to medical management of patients or procedure or complication details and had limited follow-up duration.
“The data are still not decisive,” Lima agreed. “Although, this is national data encompassing nearly a decade of inpatient hospitalizations, there are inherent limitations to what we can interpret from it. This is a retrospective analysis and therefore we don't know why patients were treated with CAS. … What would be very helpful would be a prospective randomized study comparing the two procedures.”
In the meantime, he added, “We still believe that physicians sending patients for carotid revascularization procedures should judge on an individual basis.”
The researchers are currently preparing a manuscript for publication that will include a larger dataset of patients, including patients with stage 3 and 4 CKD.
Source:
Lima FV, Yen TYM, Gruberg L. Impact of stage 5 chronic kidney disease in patients undergoing percutaneous or surgical carotid artery revascularization: insights of the Healthcare Cost and Utilization Project’s National Inpatient Sample. Presented at: TCT 2015. October 13, 2015; San Francisco, CA.
Disclosures:
- Drs. Lima and Maldonado reports no relevant conflicts of interest.
