Real-world outcomes with Solitaire are “remarkable,” one expert says, but questions remain.
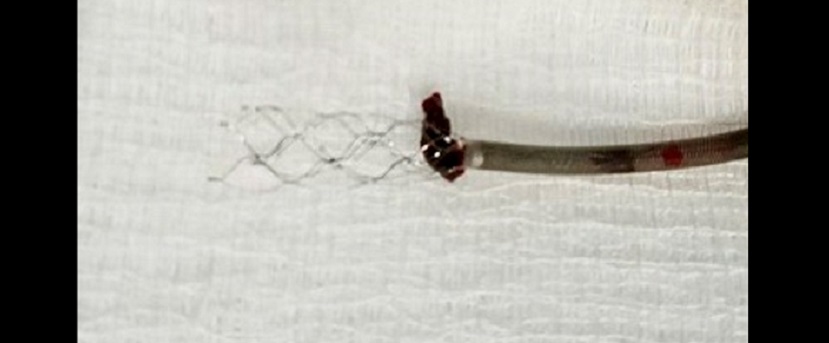
Outcomes of the Solitaire stent retriever device for mechanical thrombectomy in the real world hold up well in comparison with how it performed in clinical trials, according to an analysis published online August 22, 2017, ahead of print in Stroke.
“Since the publication of five seminal randomized clinical trials comparing mechanical thrombectomy (MT) with best medical therapy in 2015, treatment for intracranial large vessel occlusion with stent retrievers has become standard of care and has been endorsed by various guidelines around the world ≤ 6 hours from symptom onset,” write the authors, led by Nils H. Mueller-Kronast, MD (Advanced Neuroscience Network/Tenet South Florida, Delray Beach, FL).
They point out, however, that these trials “varied in their inclusion criteria, time windows, and imaging protocols, and four of the trials were stopped before the enrollment targets were reached because of efficacy.” The SEER meta-analysis was therefore undertaken, which included 401 patients from four of the trials involving Solitaire, and its results provided Level 1 evidence for the clinical use of this device.
The STRATIS (Systematic Evaluation of Patients Treated with Neurothrombectomy Devices for Acute Ischemic Stroke) registry prospectively enrolled patients treated in the United States with Solitaire and/or MindFrame Capture devices (both Medtronic) within 8 hours from symptom onset. For the new analysis, Mueller-Kronast and colleagues compared the outcomes of 984 STRATIS patients treated at 55 sites were those of the SEER meta-analysis.
Overall, outcomes among patients in the STRATIS registry were as good or better than those seen in the SEER meta-analysis.
Solitaire Use and Outcomes: STRATIS vs SEER
|
|
SEER |
STRATIS |
P Value |
|
NIHSS Score |
16.6 ± 4.9 |
17.3 ± 5.5 |
0.042 |
|
Use of IV tPA |
80.5% |
64% |
< 0.001 |
|
Onset-to-Door Time, mins |
143.5 ± 122.2 |
149.3 ± 101.0 |
0.03 |
|
Door-to-Puncture Time, mins |
122.0 ± 173.7 |
80.1 ± 49.4 |
< 0.01 |
|
Puncture-to-Reperfusion Time, mins |
45.9 ± 31.0 |
45.6 ± 29.0 |
0.74 |
|
Modified TICI ≥ 2b |
76.6% |
87.9% |
< 0.001 |
|
90-Day mRS 0-2 |
54.0% |
56.5% |
0.432 |
|
All-Cause Mortality |
12.0% |
14.4% |
0.263 |
|
Symptomatic Intracranial Hemorrhage |
2.5% |
1.4% |
0.248 |
Maxim Mokin, MD, PhD (University of South Florida, Tampa, FL), commented on the study for Neurovascular Exchange. “It is sometimes the case that clinical outcomes in real-world practice do not match the results seen in randomized trials, which tend to exclude certain population of patients,” he explained in an email.
“It is certainly remarkable,” Mokin said, “that patients treated with stent retriever thrombectomy outside of randomized trials achieved comparable clinical outcomes, namely the 56.5% rate of good clinical outcome (mRS 0-2).”
Safe and Effective First-Line Tool
According to Mokin, the study demonstrates that the Solitaire device “is safe and effective as the first-line tool of endovascular thrombectomy.” Once more, he said, the findings have “indicated that stent retriever thrombectomy is effective in the elderly.”
Another interesting finding, he noted, is that “M2 occlusions can be treated as effectively as more proximal MCA occlusions.” While the results indicated lower rates of substantial reperfusion with M2 occlusions compared with M1 occlusions (P = 0.002), rates of good functional outcome and mortality were similar for both types of occlusions (P = 0.914 and P = 0.933, respectively).
The study also reveals that “local operators tend to overestimate the reperfusion success on final angiograms, when compared to the results obtained from the core lab,” he added.
What remains unclear is how the available stent retrievers compare with each other. “There are no studies directly comparing different types of stent retrievers,” Mokin said. “Once the results of the Trevo registry are published, it will be interesting to compare the two devices. However, given different inclusion/exclusion criteria for these registries, it will be unlikely to have a reliable comparison.”
Other unanswered questions remain. “The study did not enroll patients beyond 8 hours of stroke symptom onset,” noted Mokin. “With the DAWN trial indicating the effectiveness of thrombectomy up to 24 hours, it would be important to replicate those findings in a real-world setting.”
Source:
Mueller-Kronast NH, Zaidat OO, Froehler MT, et al. Systematic evaluation of patients treated with neurothrombectomy devices for acute ischemic stroke: primary results of the STRATIS Registry. Stroke. 2017;Epub ahead of print.
Disclosures:
- This study was sponsored by Medtronic.
- Mueller-Kronast reports serving as a scientific consultant regarding trial design and conduct to Medtronic.
- Mokin reports no relevant conflicts of interest.
