Key Points:
- Researchers analyze how the effect of timing might influence results of mechanical thrombectomy
- Less favorable outcomes with longer time from CT to reperfusion, but not onset to CT
Both the time from symptom onset to imaging and the time from imaging to reperfusion are likely clinically important factors among patients who undergo mechanical thrombectomy for acute ischemic stroke. Each interval may affect outcomes in different ways, however, researchers report in a paper published online March 8, 2016, ahead of print in Stroke.
Marc Ribo, MD, of Hospital Vall d’Hebron (Barcelona, Spain), and colleagues looked at the 103 patients who underwent mechanical thrombectomy in the prospective, randomized REVASCAT trial. They defined 3 specific workflow metrics:
- Time from symptom onset to reperfusion (mean 342 minutes)
- Time from symptom onset to CT (mean 204 minutes)
- Time from CT to reperfusion (mean 138 minutes)
Median National Institutes of Health Stroke Scale (NIHSS) score at admission was 17.0. Two-thirds of patients had successful reperfusion, and 43% had a favorable outcome, defined as a modified Rankin Scale (mRS) score of 0-2.
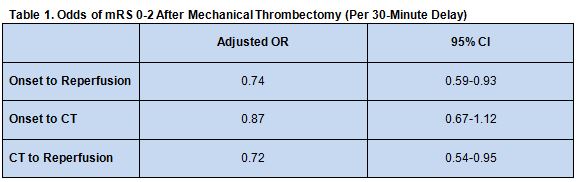
Longer time from symptom onset to reperfusion was associated with a reduced likelihood of good outcome, with the odds of achieving a good outcome reduced by 26% for every 30 min delay. While onset-to-CT time was not significantly linked with clinical outcome, longer CT-to-reperfusion time was associated with less favorable outcomes (table 1)
Subgroup analysis based on Alberta Stroke Program Early Computed Tomographic Score (ASPECTS) at admission revealed that the relationship between onset-to-reperfusion time and outcome was significant for patients with a score lower than 8 (adjusted OR 0.56; 95% CI 0.35-0.9) but not those with a score of 8 or higher (adjusted OR 0.99; 95% CI 0.68-1.44).
ASPECTS Score Could Help Guide Timing
The authors speculate that onset to CT time is an important clinical factor even though it was not apparent in this study. They explain that the lack of significant association for this interval is likely due to the fact that the REVASCAT trial employed an ASPECTS cutoff of 7 or higher. This threshold was meant to exclude patients unlikely to have good outcomes because their infarct volumes were too large. Indeed, “when analyzing according to initial ASPECTS, in patients with lower scores (ASPECTS < 8) we observed the expected negative association of time and outcome in the initial interval,” they write.
The authors argue that reducing onset-to-CT time would still likely improve outcomes by increasing the number of patients who would present with better ASPECTS score and thus be more likely to be good candidates for thrombectomy. In addition, they say, reducing CT-to-reperfusion time may improve outcomes among those who are chosen for thrombectomy.
Ribo et al also suggest that patients with an ASPECTS < 8 “may represent the group where treatment decisions should be made with the minimum available information (ASPECTS score) to save precious time to reperfusion.” Time may be less crucial among patients with higher ASPECTS scores, they say, so these patients may be more likely to benefit from thrombectomy even if time from onset to CT is unknown or have enough wiggle room that their treatment can be delayed while additional imaging studies are cone to make a more definitive diagnosis.
Source:
- Ribo M, Molina CA, Cobo E, et al. Association between time to reperfusion and outcome is primarily driven by the time from imaging to reperfusion. Stroke. 2016;Epub ahead of print.
Disclosures:
- Dr. Ribo reports no relevant conflicts of interest.