Key Points:
- Study looks at whether ICU is needed after endovascular treatment of unruptured intracranial aneurysm
- Neurologic complications rare, predicted by certain baseline factors
Not all patients undergoing coil embolization for unruptured intracranial aneurysms require monitoring in the intensive care unit (ICU) after the procedure, according to results published online July 5, 2016, in the Journal of NeuroInterventional Surgery. In fact, neurologic complications after the procedure were rare, occurring in only 3.5% of patients.
“Routine ICU admission following coil embolization of elective unruptured intracranial aneurysms is an unproven practice that persists despite advances in medical therapy and endovascular technology,” write Joseph J. Gemmete, MD, of the University of Michigan (Ann Arbor, MI) and colleagues.
The researchers conducted a retrospective cohort study looking at 311 patients (79% women) who had elective endovascular treatment of an unruptured intracranial aneurysm at their institution from 2005 and 2011. They sought to identify predictors of outcomes and conducted a cost-savings analysis comparing admission to the ICU with step-down or telemetry unit admission.
Neurologic Complications Rare
Of the 311 procedures, 61.1% involved coiling alone, 4.2% were balloon-assisted coiling, and 34.7% stent-assisted coiling. Twenty (6.4%) post-procedure complications occurred, including 11 (3.5%) neurologic complications associated with the procedure. Five patients (1.6%) suffered permanent neurologic deficit.
The researchers noted that of the 11 patients with neurologic complications, 4 had intraoperative complications and 3 had aneurysms larger than 2 cm. Among patients whose procedures were complication-free but still had neurologic complications afterward, only two had neurologic changes discovered during checks in the ICU and treatment was only altered in one case.
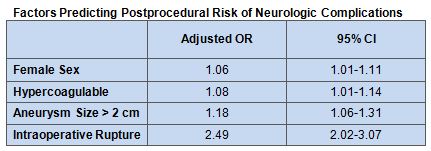
Predictors of postprocedural complications included female sex, hypercoagulability, aneurysm size larger than 2 cm, and intraoperative rupture (see table).
The cost-savings analysis showed that admission to a step-down unit with invasive line monitoring reduced costs by 32% per day compared with ICU admission. If patients were admitted to a telemetry unit without invasive monitoring, the savings increased to 57% less per day compared with the ICU.
Alternatives to ICU
In their discussion, the researchers acknowledge that patient safety is a foremost concern after undergoing coil embolization, but that cost of care must also be considered.
“ICU care remains one of the largest contributors to healthcare costs in the USA,” they write. “Patients without a complex neurologic or medical history, with a small aneurysm, or with an uncomplicated procedural course should be considered for admission to a step-down unit or telemetry bed since post-procedural complications are uncommon in these cases.”
Additionally, the investigators suggest as an alternative that patients undergoing these procedures could be monitored closely in the immediate postprocedural period of up to 4 hours.
Sources:
- Stetler WR, Griauzde J, Saadeh Y, et al. Is intensive care monitoring necessary after coil embolization of unruptured intracranial aneurysms?J NeuroIntervent Surg. 2016;Epub ahead of print.
Disclosures:
- Dr. Gemmete reports no relevant conflicts of interest.